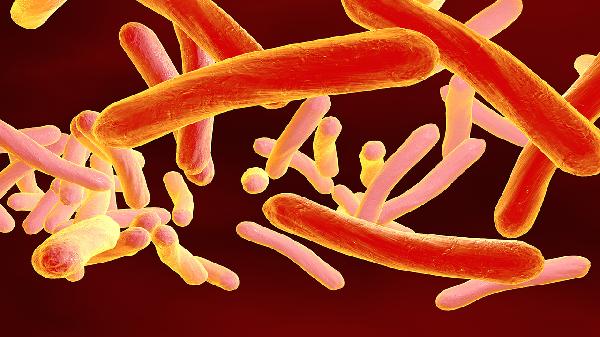
Lymphogranuloma venereum, also known as inguinal lymphogranuloma, the fourth venereal disease, tropical or climatic bubo, and Frei's disease, is one of the four major sexually transmitted diseases along with syphilis, gonorrhea, and chancroid. This disease is caused by Chlamydia, which is divided into two types: Chlamydia trachomatis and Chlamydia psittaci. The type associated with lymphogranuloma venereum is Chlamydia trachomatis. Based on serological reactions, Chlamydia trachomatis can be classified into 15 serotypes, among which the L1, L2, and L3 serotypes cause lymphogranuloma venereum.

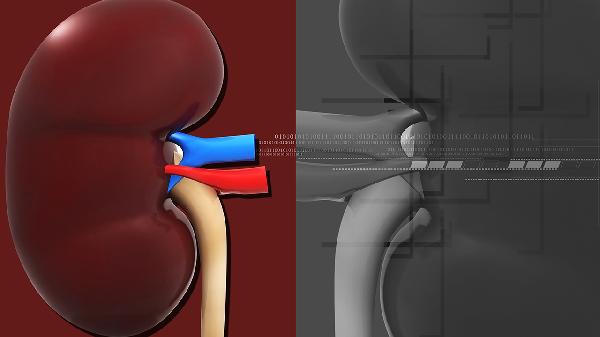
After contracting lymphogranuloma venereum, the main symptoms are swelling and suppuration of the inguinal lymph nodes. In the late stages, it can lead to many serious complications. Rectal stenosis is the most common complication, especially in women. If the lesion occurs in the urethra, it can be accompanied by urethral stenosis; if it occurs in the vagina, it can cause vaginal stenosis and even the formation of a fistula between the vagina and rectum due to perforation (referred to as a fistula in medical terms) and severe destructive damage to the vulva. The damaged genitalia can also develop cancer. Lymphogranuloma venereum does not start with these severe complications. Clinically, the disease progresses through early stages (infection, primary lesions, and skin lesions), middle stages (lymphatic dissemination, accompanied by systemic symptoms), and late stages.
1. Incubation period: Generally around 1 week.
2. Early symptoms: Initially, very small herpes and ulcers appear. In men, they commonly occur on the body of the penis, glans, coronal sulcus, and foreskin. In women, they occur in the vestibule, labia minora, vaginal opening, and around the urethral orifice. The skin lesions are usually single, sometimes multiple, with no obvious symptoms, and are often overlooked. They heal on their own within a few days without leaving scars.
3. Middle symptoms: Inguinal lymphadenitis. One to four weeks after the initial lesion, two-thirds of cases develop bilateral inguinal lymph node swelling, referred to as the "fourth venereal bubo." Initially, the lymph nodes are isolated and scattered, with hard and painful enlargement. Later, they often adhere to each other, forming a mass, with the skin surface turning purple and cyanotic. Due to the inguinal ligament separating the swollen lymph nodes, the skin appears grooved. After a few weeks, the swollen lymph nodes develop a fluctuating sensation and soften and ulcerate after one to two weeks, discharging yellow serous or bloody secretions, forming multiple fistulas resembling a "watering can." They heal after several weeks or months, leaving scars. Women rarely develop lymphadenitis because their initial lesions often occur in the lower part of the vagina, and if the infection spreads through the iliac and anorectal lymph nodes, it can cause iliac and perirectal lymphadenitis and proctitis, leading to abdominal and back pain. The onset of lymphadenitis can be accompanied by varying degrees of systemic symptoms such as fever, headache, joint pain, and hepatosplenomegaly. Sometimes, rashes like erythema multiforme or erythema nodosum may appear.
4. Late symptoms: The progression from early to late stages takes one to two years, or even several years. The main manifestations are genital elephantiasis and anorectal syndrome.
Genital elephantiasis in lymphogranuloma venereum is a severe complication that occurs in the later stages of the disease. It is caused by chronic inflammation of the lymphatic vessels leading to elephantiasis of the labia, penis, and scrotum. The skin surface may develop wart-like growths and polypoid formations, potentially leading to rectovaginal or urethral fistulas, deforming ulcers, and scars.
The anorectal syndrome in lymphogranuloma venereum is a common complication of the disease. It occurs when the inflammation spreads from the vulva to the perirectal area, causing perirectal inflammation. Bloody discharge may occur, followed by the formation of scars, leading to tubular stenosis of the lower rectum, resulting in difficulty in defecation or perianal fistulas. Due to progressive stenosis, constipation and abdominal pain may occur.
In addition to the above complications, the disease can also lead to systemic complications such as aseptic meningitis, conjunctivitis, hepatitis, and pericarditis, as well as skin lesions like erythema nodosum, erythema multiforme, scarlatiniform rash, and urticaria.